
- Offer Profile
- Our
mission is to develop science, technology, and human resources at the
interface between robotics, biological systems, and medicine.
Our goal is to produce useful, innovative research and technology as well as trained researchers fluent in both science, engineering, biological systems, and robotics.
Wearable Robotics - Exoskeletons
- The exoskeleton robot is worn by the human operator as
an orthotic device. Its joints and links correspond to those of the human
body. The same system operated in different modes can be used for three
fundamental applications: a human-amplifier assistive device sharing a
portion of the external load with the operator, haptic device, and automatic
physiotherapy.
The current research effort with the upper limb exoskeleton is focused on the developing human machine interface (bioport) at the neuromuscular level using EMG (electromyography) signals as the primary command signal to the system. The research effort with the lower limb exoskeleton is focused on developing a semi active system for improving the ability of the operator to carry a payload. 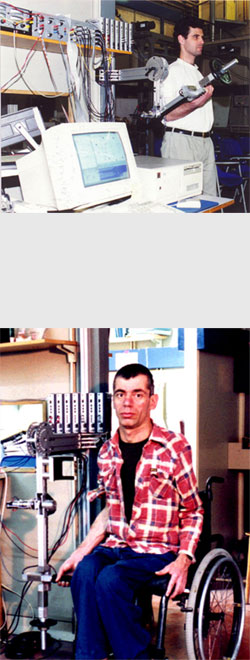
Exoskeleton Prototype 1 (EXO-UL1)
- The first exoskeleton mechanism consisted of a two-link,
two-joint device corresponding to the upper and the lower arm and to the
shoulder and elbow joints of the human body. The system included a weight
plate (external load) that can be attached to the tip of the exoskeleton
forearm link. The mechanism was fixed to the wall and positioned parallel to
the sagittal plane of the operator. The human/exoskeleton mechanical
interface included the upper arm bracelet, located at the upper arm link,
and a handle grasped by the operator. This two-joint mechanism was used as a
one-degree of freedom system by fixing the system shoulder joint at specific
angles in the range of 0-180 Deg. The elbow joint was free to move in an
angle range of 0-145 Deg, and included built-in mechanical constraints which
kept the exoskeleton joint angle within the average human anthropometric
boundaries. Since the human arm and the exoskeleton were mechanically linked
the movements of the forearms of both the human and the exoskeleton were
identical.
The basic purpose of the exoskeleton system as an assistance device is to amplify the moment generated by the human muscles relative to the elbow joint, while manipulating loads. The exoskeleton's elbow joint was powered by a DC servo motor (ESCAP-35NT2R82) with a stall torque of 360 mNm equipped with a planetary gearbox (ESCAP-R40) with a gear ratio of 1:193 and a maximal output torque of 40 Nm. An optical incremental shaft encoder (HP HEDS 5500) with 500 lines was attached to the motor shaft. Due to the encoder location and the high gear ratio, the practical encoder's resolution for measuring the joint angle was 0.0036 Deg. This setup incorporated a DC motor with the highest torque-to-weight ratio that was available on the commercial market at that time with a power consumption that could be provided by a battery. A high energy density of the power supply and an actuator with a high torque-to-weight ratio are two key features of the exoskeleton system as a self contained mobile medical assistance device for the disabled community. Limits imposed by present technology on these two key components along with design requirements for developing a compact system with a potential of serving as a medical assistance device for disabled person restricted the payload to be 5 Kg. However, this biomedical oriented design does not restrict the generality of the exoskeleton concept or its operational algorithms. Using other actuation systems, like hydraulic system increases the load capacity substantially.
The exoskeleton forearm was extended by a rod with a special connector for attaching disk-type weights (external load). Two force sensors (TEDEA 1040) were mounted at the interfaces between the exoskeleton and the tip carrying the external load and between the exoskeleton and the human hand. The first load cell, inserted between the rod holding the external load and the exoskeleton forearm link, measured the actual shear force, normal to the forearm axis, applied by the external load. The second load cell was installed between the handle grasped by the human hand and the forearm link of the exoskeleton. This load cell measured the shear force applied by the operator to the handle. Multiplying the sensors' measurements by the corresponding moment arms indicated the moments applied by the weights and by the human hand relative the elbow joint.Surface EMG electrodes (8 mm Ag-AgCl BIOPAC - EL208S) were attached to the subject’s skin by adhesive disks for measuring the EMG signal of the Biceps Brachii and Triceps Brachii medial-head muscles. The signals were gained by EMG amplifiers (BIOPAC - EMG100A) using a gain factor in the range of 2000-5000 (depending on the subject). The EMG signals and the load cell signal were acquired by an A/D convector (Scientific Solution Lab Master 12 bit internal PC card) with a 1 kHz sampling rate, whereas the encoder signals were counted by custom-made hardware. The entire data set was recorded simultaneously and stored, for later off-line analysis and simulation.
A special real-time software, for operating the system, was written in C and run on a PC-based platform. The software was composed of three main modules. The first module dealt with the hardware/software interface. It controlled the interaction between the PC and the external motor driver and the sensors, through a D/A and an A/D card. The second module included the automatic code generated by the MATLAB - Simulink Real-Time toolbox. The third module was the user interface module which allowed to set various run time operational parameters. All the modules were compiled and linked for generating an efficient real-time software.

Exoskeleton Prototype 2 (EXO-UL3)
- The second exoskeleton mechanism consisted of a
three-link, two-joint device corresponding to the upper and the lower arm
and to the shoulder and elbow joints of the human body. The system included
a weight plate (external load) that can be attached to the tip of the
exoskeleton forearm link. The mechanism was fixed to the wall and positioned
parallel to the sagittal plane of the operator. The human/exoskeleton
mechanical interface included the upper arm bracelet, located at the upper
arm link, and a handle grasped by the operator. This two-joint mechanism was
used as a two-degree of freedom system. The elbow and the shoulder joints
were free to move in their anatomical range of motion. The mechanism
included built-in mechanical constraints which kept the exoskeleton joint
angles within the average human anthropometric boundaries. Since the human
arm and the exoskeleton were mechanically linked the movements of the
forearms and the upper arm of both the human and the exoskeleton were
identical.
The basic purpose of the exoskeleton system as an assistance device is to amplify the moment generated by the human muscles relative to the elbow joint, while manipulating loads. The exoskeleton's elbow and shoulder joints were powered by a DC servo motor (ESCAP-35NT2R82) with a stall torque of 360 mNm equipped with a planetary gearbox (ESCAP-R40) with a gear ratio of 1:193 and a maximal output torque of 40 Nm. An optical incremental shaft encoder (HP HEDS 5500) with 500 lines was attached to the motor shaft. Due to the encoder location and the high gear ratio, the practical encoder's resolution for measuring the joint angle was 0.0036 Deg. This setup incorporated a DC motor with the highest torque-to-weight ratio that was available on the commercial market at that time with a power consumption that could be provided by a battery. A high energy density of the power supply and an actuator with a high torque-to-weight ratio are two key features of the exoskeleton system as a self contained mobile medical assistance device for the disabled community. Limits imposed by present technology on these two key components along with design requirements for developing a compact system with a potential of serving as a medical assistance device for disabled person restricted the payload to be 5 Kg. However, this biomedical oriented design does not restrict the generality of the exoskeleton concept or its operational algorithms. Using other actuation systems, like hydraulic system increases the load capacity substantially.
The exoskeleton forearm was extended by a rod with a special connector for attaching disk-type weights (external load). Four force sensors (TEDEA 1040) were mounted at the interfaces between the exoskeleton and the operator, one at the tip carrying the external load, two between the exoskeleton and the human hand and one at the interface between the upper arm and the exoskeleton. The first load cell, inserted between the rod holding the external load and the exoskeleton forearm link, measured the actual shear force, normal to the forearm axis, applied by the external load. The other load cells were installed between the handle grasped by the human hand and the forearm link of the exoskeleton and between the upper arm bracelet and the exoskeleton upper link. These load cells measured the shear forces applied by the operator to the mechanism. Multiplying the sensors' measurements by the corresponding moment arms indicated the moments applied by the weights and by the human arm relative the elbow and the shoulder joints.Surface EMG electrodes (8 mm Ag-AgCl BIOPAC - EL208S) were attached to the subject’s skin by adhesive disks for measuring the EMG signal of the Biceps Brachii and Triceps Brachii medial-head muscles. The signals were gained by EMG amplifiers (BIOPAC - EMG100A) using a gain factor in the range of 2000-5000 (depending on the subject). The EMG signals and the load cell signal were acquired by an A/D convector (Scientific Solution Lab Master 12 bit internal PC card) with a 1 kHz sampling rate, whereas the encoder signals were counted by custom-made hardware. The entire data set was recorded simultaneously and stored, for later off-line analysis and simulation.
A special real-time software, for operating the system, was written in C and run on a PC-based platform. The software was composed of three main modules. The first module dealt with the hardware/software interface. It controlled the interaction between the PC and the external motor driver and the sensors, through a D/A and an A/D card. The second module included the automatic code generated by the MATLAB - Simulink Real-Time toolbox. The third module was the user interface module which allowed to set various run time operational parameters. All the modules were compiled and linked for generating an efficient real-time software.

Exoskeleton Prototype 3 (EXO-UL3)
- Integrating human and robot into a single system offers
remarkable opportunities for creating a new generation of assistive
technology for both healthy and disabled people. Humans possess naturally
developed algorithms for control of movement, but they are limited by their
muscle strength. In addition, muscle weakness is the primary cause of
disability for most people with neuromuscular diseases and injuries to the
central nervous system. In contrast, robotic manipulators can perform tasks
requiring large forces; however, their artificial control algorithms do not
provide the flexibility to perform in a wide range of fuzzy conditions while
preserving the same quality of performance as humans. It seems therefore
that combining these two entities, the human and the robot, into one
integrated system under the control of the human, may lead to a solution
that will benefit from the advantages offered by each subsystem.
The exoskeleton robot, serving as an assistive device, is worn by the human (orthotic) and functions as a human-amplifier. Its joints and links correspond to those of the human body, and its actuators share a portion of the external load with the operator. One of the primary innovative ideas of the proposed research is to set the Human Machine Interface (HMI) at the neuromuscular level of the human physiological hierarchy using the body's own neural command signals as one of the primary command signals of the exoskeleton. These signals will be in the form of processed surface electromyography (sEMG) signals, detected by surface electrodes placed on the operator's skin. The proposed HMI takes advantage of the electro-chemical-mechanical delay, which inherently exists in the musculoskeletal system, between the time when the neural system activates the muscular system and the time when the muscles generate moments around the joints. The myoprocessor is a model of the human muscle running in real-time and in parallel to the physiological muscle. During the electro-chemical-mechanical time delay, the system will gather information regarding the physiological muscle’s neural activation level based on processed sEMG signals, the joint position, and angular velocity, and will predict using the myoprocessor the force that will be generated by the muscle before physiological contraction occurs. By the time the human muscles contract, the exoskeleton will move with the human in a synergistic fashion, allowing natural control of the exoskeleton as an extension of the operator's body.
The goal of this research is to design, build, and study the integration of a powered exoskeleton controlled by myosignals for the human arm. The research will pursue this goal through several objectives: (i) developing an 8 degrees of freedom powered anthropomorphic exoskeleton for the arm, including grasping/releasing; (ii) setting the HMI at the neuromuscular level by using processed sEMG signals as the primary command signal to the exoskeleton system; (iii) developing muscle models (myoprocessor) for predicting the human arm joints' torques; (iv) developing control algorithms that will fuse information from multiple sensors and will guarantee stable exoskeleton operation; (v) evaluating the overall performance of the integrated system using standardized arm/hand function tests. These goals and objectives will be pursued using several experimental protocols aimed at developing the myoprocessors and evaluating the exoskeleton performance. The proposed experimental protocol includes only healthy subjects as the first step in a long-term goal aimed to evaluate the exoskeleton performance with disabled subjects suffering from various neurological disabilities, such as stroke, spinal cord injury, muscular dystrophies, and other neurodegenerative disorders.It is anticipated that the proposed research will advance the current knowledge in the field of modeling human muscles and their mathematical formulation. This knowledge will be further used to create a novel HMI and will permit a better understanding of the interaction between human and robot at the neural level. In addition, the proposed research will provide a tool and fundamental understanding regarding the development of an assistive technology for improving the quality of life of the disabled community. The proposed scientific activity will promote interdisciplinary collaboration between students and faculty members from the fields of electrical engineering, mechanical engineering, bioengineering, and rehabilitation medicine.
Surgical Robotics
- Surgical robotics is the application of advanced technology to minimally invasive surgery (MIS) and open surgery training and procedures. The research is focused on following trusts: surgical robots, teleoperation, objective assessment of surgical performance, simulation, and the biomechanics of soft tissue that are related MIS and open procedures.

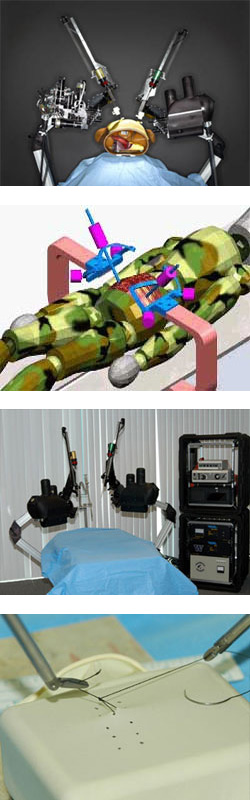
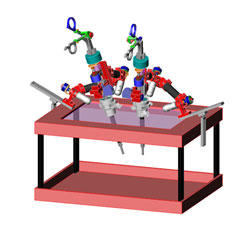
Raven IV - Colaborative Surgery
- Surgery is traditionally conducted as a collaborative
effort including a prime surgeon, an assistant along with scrub and
circulation nurses. The introduction of surgical robotics into the operating
room (OR) change the dynamics and the type of interaction that was perfected
over decades. For the clinically approved surgical robotic systems the
surgeon is still in the OR but he or she is physically removed from the
patient. Using a surgical consoles the surgeon may teleoperate up to three
tools and a camera are. The assistant may use another surgical console or
physically interact with the robot by replacing tools or interacting with
tissues using manually operated tools.
In order to reproduce the originally dynamics of two surgeons interacting with the surgical site using a robotic system, four dexterous arms accounted for the four arms of the two surgeons along with two pairs of eyes are needed. Raven IV is a surgical robotics system that was developed at the University of California – Santa Cruz which includes four robotics arms and 2 cameras. The system facilitates a collaborative effort of two surgeons interacting with the surgical site in teleportation. Each surgical arms is based on a spherical mechanisms with a remote center located at the point of entry of the tool into the human body. A detailed optimization of the surgical robotics arms was conducted to minimize the footprint of the system in the operational field while maximizing the manipulability of the arms in their shared workspace. The system architecture allows two surgeons in two remote locations to connect via commercially available internet connection using a UDP protocol using a unique software client interface and teleoperate the surgical robots in a master/slave configuration. Initial teleoperation experiments conducted within the continental US from several remote locations allowed two surgeons, each one controlling a set of two arms, to complete fundamental laparoscopic surgery (FLS) tasks collaboratively while using sampling rate of 1 kHz.
Collaborative surgery will continue to be the preferred modus operatndi in surgery and Raven IV demonstrated its capability to support this mode using a surgical robotic system.
Raven - A Surgical Robotic System
- The individual soldier remains the most valuable asset of
the military, and in spite of the current emphasis on the threat of weapons
of mass destruction (WMD) and biological warfare (BW), attending to the
soldier's needs when they become a casualty remains a top priority. Very
little has changed in terms of the needs of the wounded soldier at the
far-forward battlefield, especially during the "golden hour''. What has
changed is the technology to significantly bring immediate care to the
casualty. There is a significant opportunity to save the lives of soldiers
by using forward deployed telesurgical capabilities to control the
consequences of abdominal vascular injury.
The surgical robots resulting from DARPA research now being deployed and FDA approved are very exciting developments, but share significant limitations: bulky envelope, lack of haptic (force) feedback, and high costs. In selecting the appropriate mechanism for a surgical robot we must incorporate knowledge of the surgical task, the surgical environment, tool kinematics and dynamics, and properties of actuators, transmissions, and structural elements.
Objective/ Hypothesis
We believe the design approach of todays surgical robots, and their consequent size and weight, prevent the effective deployment for military needs and that a new class of surgical robotic mechanisms can be developed which will be dramatically smaller than existing designs. We will test this hypothesis by developing design theory, and prototype designs, and quantitatively evaluate them against an extensive database of force and displacement measurements in surgery.
Specific Aims/Objectives- Measure all relevant forces and displacements in actual surgery in experimental animals in procedures, sub-procedures, and skills most relevant to abdominal vascular trauma in combat casualty care.
- Study candidate mechanisms, and develop computerized design tools which translate quantitative surgical requirements into mechanism parameters.
- Design and prototype a new, dual arm teleoperated surgical manipulator, supporting the motions and forces/torques obtained in objective 1, using the methods of objective 2.
- Evaluate the performance of the prototype in experimental animal surgery
Study Design
The four-year project included four parallel tasks aimed at the objectives above. Mechanism design was closely based on measurements of the physics of actual surgery. Performance of the prototype was evaluated in experiments and animal surgeries covering atraumatic control of vessels, cautery, tissue welding, suturing, and repair of vessel injuries to include: side cut vessel, clean cut vessel, ragged, torn vessel, ragged torn vessel with gap between ends.
Relevance to Military Health Issues
The past 10 years have seen the concept of robot assisted surgery go from advanced DARPA-funded prototypes to FDA approved commercial technology. However, the DOD's original vision of forward-deployed combat casualty care is still not possible. Today's commercial and research surgical robots are much too large to be deployed inside a vehicle. Our proposed design methods will dramatically reduce the military disadvantages of existing commercial and research surgical robots through two novel aspects. 1) mechanical design requirements would be derived from our quantitative measurements of actual surgery so that no excess capability will be designed into the system. and 2) we will move the actuation point closer to the surgical site --- dramatically reducing the volume and weight while smoothing and speeding up the motion response. These improvements will allow a surgical robot to be used to save lives in the cramped space of a forward deployed armored personnel carrier for the first time.
Teleoperation Studies
Raven as a surgical robotic platform was subject of an extensive effort of deploying it in extreme environments and teleoperate it form large distance while utilizing wired and wireless communication channels.
Red DRAGON (Edge)
- With the development of new technologies in surgery,
minimally invasive surgery (MIS) has drastically improved the way
conventional medical procedures are performed. However, a new learning curve
has resulted requiring an expertise in integrating visual information with
the kinematics and dynamics of the surgical tools.
The Red DRAGON is a multi-modal simulator for teaching and training MIS procedures allowing one to use it with several modalities including: simulator (physical objects and virtual objects) and an animal model. The Red DRAGON system is based on a serial spherical mechanism in which all the rotation axes intersect at a single point (remote center) allowing the endoscopic tools to pivot around the MIS port. The system includes two mechanisms that incorporate two interchangeable MIS tools. Sensors are incorporated into the mechanism and the tools measure the positions and orientations of the surgical tools as well as forces and torques applied on the tools by the surgeon.
The design is based on a mechanism optimization to maximize the manipulability of the mechanism in the MIS workspace. As part of a preliminary experimental protocol, five expert level surgeons performed three laparoscopic tasks – a subset of the Fundamental Laparoscopic Skill (FLS) set as a baseline for skill assessment protocols. The results provide an insight into the kinematics and dynamics of the endoscopic tools, as the underlying measures for objectively assessing MIS skills.

Trauma Pod - Phase 1 The Operating Room of the Future
- Background The Trauma Pod (TP) vision is to
develop a rapidly deployable robotic system to perform critical acute
stabilization and/or surgical procedures, autonomously or in a teleoperative
mode, on wounded soldiers in the battlefield who might otherwise die before
treatment in a combat hospital could be provided.
Methods In the first phase of a project pursuing this vision, a robotic TP system was developed and its capability demonstrated by performing selected surgical procedures on a patient phantom.
Results The system demonstrates the feasibility of performing acute stabilization procedures with the patient being the only human in the surgical cell. The teleoperated surgical robot is supported by autonomous robotic arms and subsystems that carry out scrub-nurse and circulating-nurse functions. Tool change and supply delivery are performed automatically and at least as fast as performed manually by nurses. Tracking and counting of the supplies is performed automatically. The TP system also includes a tomographic X-ray facility for patient diagnosis and two-dimensional (2D) fluoroscopic data to support interventions. The vast amount of clinical protocols generated in the TP system are recorded automatically.
Conclusions Automation and teleoperation capabilities form the basis for a more comprehensive acute diagnostic and management platform that will provide life-saving care in environments where surgical personnel are not present.

Motorized Endoscopic Grasper (MEG)
- Accurate biomechanical characteristics of tissues is
essential for developing realistic virtual reality surgical simulators using
haptic devices. Surgical simulation technology has progressed rapidly but
without a large database of soft tissue mechanical properties with which to
incorporate. In addition, the majority of the research that has been done on
measuring mechanical properties of abdominal soft tissues was performed in
vitro, on animals and cadavers. As simulation technologies continue to be
capable of modeling more complex behavior, a tissue property database needs
to be developed to fill this gap. This problem has been addressed in recent
work with a variety of tools and techniques.
We have adapted our previous design for the force-reflecting endoscopic grasper (FREG) to a motorized endoscopic grasper (MEG) that uses a brush DC motor instead of a voice-coil actuator. The motor is attached to a capstan that drives a cable and partial pulley. The pulley is attached to a ball joint that converts the rotational motion of the motor and pulley to a linear translation. The motor is capable of producing 29 mNm of continuous torque, but it is coupled with a 19:1 planetary gearhead and partial pulley that increase the torque to 3.98 Nm. This torque is equivalent to 52 N of grasping force applied by a surgeon on an endoscopic grasper's finger loops, close to the maximum value applied by surgeons in our previous work. Standard laparoscopic instruments can be attached to the base plate mount and inserted into the ball joint. Two strain gage force sensors are embedded in the pulley to provide accurate grasping force measurement. A digital encoder, attached to the motor, measures position. Computer control is provided real-time via a PC using a PD controller implemented in Simulink and custom dSPACE user interface. The MEG is a hand-held device that weighs 0.7 kg (including grasper) and can be inserted into the body through regular endoscopic ports to perform computer-controlled dynamic and static uniaxial compressive displacements (position-controlled) of soft tissues.
The MEG was used to measure biomechanical characteristics of porcine tissues in vivo of the following organs: liver, spleen, lung, stomach, small bowel, and colon through a series of static and dynamic grasping tests. The resulting force-deformation data were transformed to stress-strain, which were further processed to obtain elastic modulus, creep time constant, stress relaxation time constant. Tissue types exhibited significant differences in properties. Tissue property inhomogeneity was also studied.
The MEG will help provide realistic data for surgical simulation and corroborate the results of other researchers. Future work will be to compare in vivo MEG data with in vitro MEG and universal testing machine data to observe the changes in tissue mechanical properties postmortem.

Blue DRAGON
- The BlueDRAGON is a system for acquiring the kinematics
and the dynamics of two endoscopic tools along with the visual view of the
surgical scene. The system includes two four-bar passive mechanisms attached
to endoscopic tools. The four bar mechanisms translate the tool's rotation
around the pivot point located in the port into the mechanism's joints
incorporating position sensors. These translation is enabled when the base
axes and the tool's shaft axis intersect the port's pivot point. Moreover,
the mechanism's axes alignment prevented any additional moments applied on
the skin and internal tissues except the ones that are generated
intentionally by using the tools. The gravitational forces applied on the
surgeon's hand when the mechanism is away from its neutral position are
compensated by an optimized spring connecting the bases and the first two
coupled links.
The two mechanisms are equipped with three classes of sensors: (i) position sensors (multi turn potentiometers - Midori America Corp.) are incorporated into four of the mechanisms' joints for measuring the positions, the orientations and the translation of the two instrumented endoscopic tools attached to them. In addition, two linear potentiometer (Penny & Giles Controls Ltd.) that are attached to the tools' handle are used for measuring the endoscopic handle and tool tip angles; (ii) three-axis force/torque (F/T) sensors (ATI-Mini sensor) are located at the proximal end of the endoscopic tools' shaft, as well as force sensors inserted into the tools' handles for measuring the grasping forces at the hand/tool interface and (iii) contact sensors providing binary indication of any tool/tissue contact. Data measured by the BlueDRAGONs' sensors are acquired using two 12-bit National Instruments USB A/D cards sampling the 26 channels (3 rotations, 2 translations, 1 tissue contact, and 7 channels of forces and torques from each instrumented grasper) at 30 Hz. In addition to the data acquisition, the synchronized view of the surgical scene is incorporated into a graphical user interface displaying the data in real-time.
Multidimensional Topics
- The following list defines a cluster of research and educational efforts in Bioengineering, and Biomedical Engineering with a special focus on the human machine interface.
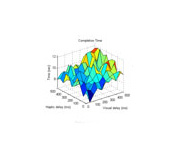
Constant Visual and Haptic Time Delays in Teleoperation Control Stability and Human Operator Performance in a Simulated Virtual Reality Teleoperation
- The goal of this research effort is to study the effects of haptic and visual time delays on human operators performance in simulated teleoperation tasks. Non synchronized haptic and visual time delays are typical to any teleoperation task utilizing communication networks such as the internet (wired and wireless).

Central Venous Catheter - Training Program
- Central venous catheters (CVC) are catheters inserted into the major deep (also termed central) veins of the neck, chest, or abdomen. CVCs are used for monitoring hemodynamic status, for administering medications or parenteral nutrition that require a high flow system for mixing, or for dialysis. Placement of a CVC is therefore one of the most common procedures performed in the care of high-risk patients. This program is designed to rapidly orient medical students, residents, attending physicians, and nurses to a standardized method of central venous catheter (CVC) placement. The program was developed as part of a collaborated efforts with Dr. Mika Sinanan and Dr. Sara Kim form the Institute for Simulation and Interprofessional Studies (ISIS) at the University of Washington.

Snowboarding in Virtual Reality -
An Instrumented Snowboard Integrated with Microsoft XBox- A real snowboard was attached to a suspended mechanical platform allowing a user standing on it and roll the board. Sensors including position sensors attach to the board as well as multi axes accelerometer attached to the user belt allowed sensory inputs to the Xbox game pad. The user wearing head mounted display (HMD) can play any board based Xbox game such as Amped using his or her body motion.

Total Hip Joint Replacement Utilizing a Minimally Invasive Surgical Approach Implants
- A prototype implant for THR was developed along with the
surgical tools, and the surgical technique for minimally-invasive. Utilizing
only two keyholes, the implants are inserted into the hip joint and expanded
in place internally. While THR is the current focus, the concept is
applicable to other joints, as well as to other surgical procedures, such as
fracture fixation surgery.
The implant for performing total hip joint replacement using minimal invasive technique (40mm incision vs. 200-300mm) comprises of a socket, a stem, and a unique set of tools.

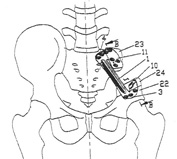
Ilio - Lumber Fixation Device
- The purpose of this implant is to generate an artificial connection between the lumbar spine (L4, L5) and the Sacrum, through the Ilium, in cases where the anatomical link between L5 and the Sacrum was damaged by a trauma. The implant/Ilium interface provides superior mechanical connection compared to other implants which interact directly with the Sacrum. The Ilium connection eliminates a potential damage to the nerves which are routed through the Sacrum.
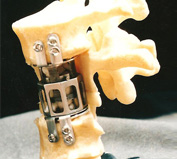
Intra-Vertebral Implant
- The purpose of this implant is to support and stabilize the spinal column in cases of total or partial veretebroctomy. The adaptive geometry of the implant can be adjusted to various anatomies. The length of the implant can be changed after the implant was set in place by a special tool allowing its two parts to move vertically with respect to each other. The space between the top and the bottom plates can be filled with segments of bone that will grow and fuse the top and the bottom vertebra.
Pelvic Plates
- The purpose of this implant is to replace parts of the pelvic that are removed in surgery. Given the patient anatomy, a deformable thin plate is used by the surgeon as a template to define the appropriate shape of the plate during surgery. The implant is plastically deformed to match the modified geometry of the template prior to fixing it to the bone.
Hidden Markov Model Toolbox for MATLAB
- The Hidden Markov Model (HMM) Toolbox for Matlab is a library of functions (M-files) that were written in Matlab's script language implementing both the discrete version (DHMM) and the continuous version (CHMM) of the HMM.